Dilution Dysfunction: Human Error and System Failures
Automated disinfectant dispensers are widely used in healthcare settings, and their reliability is paramount. However, several research studies have shown that automated dilution systems can deliver inaccurate levels of disinfectant concentrations.1,2,3 A recent study by Dr. Curtis Donskey et al. emphasizes the urgent need for improved monitoring to ensure that correct disinfectant concentrations are delivered.
Study overview
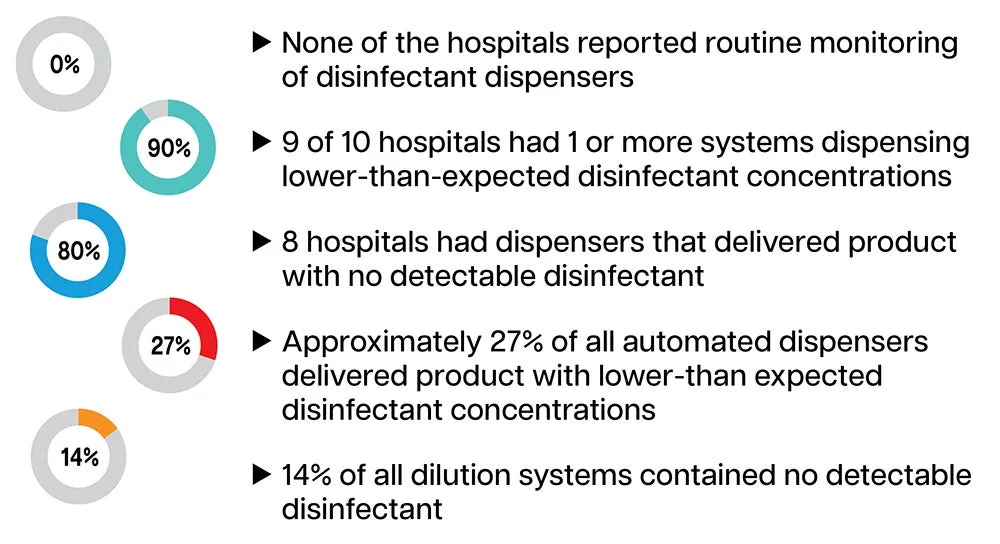
The study by Donskey et al. evaluated automated disinfectant dispensing systems in 10 hospitals across four healthcare systems. Researchers collected samples from dispensers and in-use disinfectant buckets, focusing on quaternary ammonium disinfectant cleaners and a peracetic acid/hydrogen peroxide product. The findings were concerning: 90% of hospitals had at least one dispenser delivering lower-than-expected disinfectant concentrations, and 14% of the dispensed product had no detectable disinfectant. When disinfectant levels are undetectable or below the expected concentration, there is not enough disinfectant to effectively kill pathogens, potentially leading to non-compliance with disinfection protocols. Low or undetectable levels of disinfectant can compromise the disinfectant's efficacy and increase the risk of hospital-acquired infections (HAIs) for patients.
Key study findings
Below are my top four takeaways from the study.
-
Potential Lack of Routine Monitoring and Testing: The study participants did not disclose the frequency of routine maintenance and testing of disinfectant dispensers for accurate dilution. A potential lack of oversight could have contributed to significant discrepancies in the concentrations of the disinfectant dispensed for use.
-
Inaccurate Disinfectant Levels: About 27% of dilution systems dispensed lower-than-expected concentrations, with 14% having no detectable disinfectant. This resulted in inefficient disinfection against two major pathogens of concern: methicillin-resistant Staphylococcus aureus (MRSA) for the quaternary ammonium product and Clostridioides difficile (C. diff) for the peracetic acid product.
-
Human Factors Engineering: The absence of disinfectant was often due to human error, such as incorrect connection of concentrate containers or failure to change empty containers. This highlights the importance of using technology and processes that are compatible with human capabilities/limitations to improve safety, usability, and efficiency.
-
Improvement with Intervention: After intervention at one hospital using a quaternary ammonium disinfectant, the accuracy of disinfectant concentrations improved significantly. The intervention was multifaceted and included some key components, such as:
-
Developing a Standard Operating Procedure (SOP) for use of the dispensing system
-
Educating environmental service (EVS) supervisors and staff
-
Standardizing the placement of disinfectants in dispensers to reduce end-user confusion regarding the selection of the accurate disinfectant
-
Monitoring the dispensed product by having EVS supervisors use test strips to check disinfectant concentrations monthly and each time the concentrate container was changed, recording results on a spreadsheet. Additionally, Infection Control conducted intermittent monitoring of quat concentrations, providing feedback to the EVS director, and presenting findings at quarterly meetings.
-
Recommendations for Infection Prevention & Control (IPC)
Inaccurate disinfectant concentrations can compromise patient safety by reducing the efficacy of disinfection against pathogens. To address this concern, Infection Preventionists (IPs) should advocate for the following measures:
- Increased monitoring and testing: Develop SOPs for use of dispensing systems and implement intervention strategies, such as increased monitoring and testing, to confirm the accuracy of disinfectant concentrations. Regular tests with pH strips that occur monthly or with each change of the concentrate container, for example, can help monitor the concentration of disinfectant being delivered.
- Training, education and competency: Provide comprehensive training for EVS personnel on the proper use and maintenance of disinfectant dispensing systems.
- Error reporting: Establish a system for reporting and addressing discrepancies in disinfectant appearance and odor. Be sure to notify the facility IP as this could be a factor for consideration in HAI surveillance.
- Consider ready-to-use (RTU) disinfectants: Ready-to-use (RTU) disinfectants can provide efficiency and compliance benefits over dilutable disinfectants. Since RTU products require no mixing or dilution, they reduce the time and effort needed from EVS teams, ensure the correct disinfectant concentrations for optimal effectiveness, and simplify the process of competency assessment.
Conclusion
IPC is a cornerstone of patient safety, and effective disinfection practices are foundational in healthcare settings. Dr. Donskey et al.’s recent study emphasizes the critical need for consistent checks on automated disinfectant dispensing systems to guarantee their proper operation and correct usage. By enhancing oversight and implementing routine monitoring and testing of dilution systems, or by opting for simplified and standardized RTU disinfectants, healthcare facilities can help ensure effective disinfection practices, ultimately improving patient safety and infection control.
For more detailed information, please refer to the full article in Infection Control & Hospital Epidemiology.4
Share this article
About the Author

More from the Clorox Pro Blog

References
- Boyce JM, Sullivan L, Booker A, Baker J. Quaternary ammonium disinfectant issues encountered in an environmental services department. Infect Control Hosp Epidemiol 2016;37:340-2.
- O'Neill C, Ramage L, Wyatt L, Ballantyne L. Quality control is indispensable for automated dilution systems with accelerated hydrogen peroxide. Can J Infect Control 2009;24:226-8.
- Hawley B, Casey M, Cummings KJ, Edwards N, Johnson A, Cox-Ganser J; National Institute of Occupational Safety and Health. Evaluation of exposure to a new cleaning and disinfection product and symptoms in hospital employees. NIOSH health hazard evaluation report, HHE 2015-0053-3269, 2017. Available at: https://stacks.cdc.gov/view/cdc/44556. Accessed March 15, 2024.
- Cadnum JL, Kaple CE, Eckstein EC, et al. Dilution dysfunction: evaluation of automated disinfectant dispenser systems in 10 hospitals demonstrates a need for improved monitoring to ensure that correct disinfectant concentrations are delivered. Infection Control & Hospital Epidemiology. Published online 2024:1-4. doi:10.1017/ice.2024.148